Wisconsin Model
Program Goals & Key Components
The WI DOC program’s overarching goals include a reduction in opioid-related overdoses, relapse, and violations of supervision. The department developed the program based on the following key components.
- Program provides 12 months of Medicated-assisted treatment (MAT) and other treatment services.
- Participants must reside in a certain geographic area of the state
- Individuals releasing from prison must have completed AODA treatment services in the institution
- Individuals releasing from prison will receive their first MAT up to 7 days prior to their release
- Participants are assigned to a specially trained MAT agent
- Participants must volunteer to participate
Length of Program
The Wisconsin Department of Corrections chose a program model that would last 12 months. After consultation with other states and other MAT programs that last six months, we learned many of those programs felt six months was not long enough to achieve their desired outcomes. We understood the challenges that a 12-month program could present, but we believed this approach best suited our long- and short-term goals. We also recognized that some participants would complete the program in less than 12 months based on a variety of reasons including early discharge from supervision. Injections of Naltrexone (Vivitrol) would be delivered up to seven days prior to the participant’s release from a jail or prison for the following reasons:
- Reduce likelihood of overdose prior to returning to their homes
- Provide an observation period for adverse reactions to the medication
- Cognitive behavioral treatment would be the emphasis of this program as the treatment would provide the tools for participant’s success after the use of Naltrexone has been completed. The results of the AODA/substance use disorder (SUD) assessment would determine treatment services: outpatient programming, intensive outpatient programming, aftercare, or relapse. These services will typically last four to six months for successful completion.
Treatment and Counseling
From the onset, participants in this program are advised that enrollment is strictly voluntary. All volunteer participants go through a medical screening process and an AODA/SUD assessment to determine treatment needs and level of care.
- Use of Naltrexone – no other forms of MAT
- Completion of cognitive based AODA counseling
- Where available, completion of "Thinking for Change", a program designed to address criminal and antisocial cognitions, beliefs, and companions.
The Wisconsin Division of Community Corrections does not employ treatment and counseling staff to provide direct services to offenders. As a result, contracts for the various medical, treatment, and counseling services would be required to deliver the related services. Contracts would emphasize:
- Evidence based practices - Risk, Needs, Responsivity
- Cognitive behavioral therapy - curriculum, role play, skill practice
Entry Points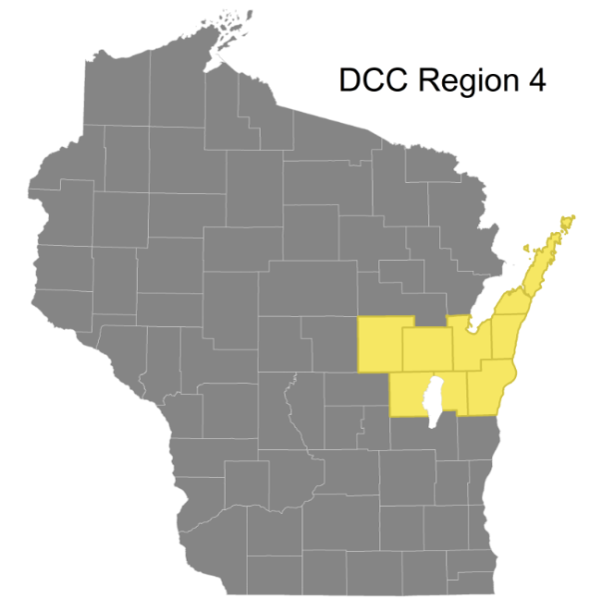
We focused our efforts on a subset of eight prisons in our Division of Adult Institutions (DAI) system to pilot this program. These institutions were selected based upon current level of treatment services offered, health services staff availability for MAT, and in some cases, proximity to the inmate’s release plan residency.
Our adult Division of Community Corrections (DCC) system is divided into eight Regions. We chose the eight counties that make up Region 4 (Northeast Wisconsin). This geographic area was selected after we studied opioid violations, use, and criminal prosecution trends.
Program Referrals
Division of Adult Institutions (DAI)
- Health Services involvement
- Medical screening form and criteria were developed and established in accordance with medical guidelines for Vivitrol.
- Informed consents for offenders were created.
- A process for creating communication between departments was developed to include health services unit, pharmacy, social services, and the probation and parole agent.
- Health services unit staff were trained on the pilot program process as well as the Vivitrol medication.
- Ultimately it was determined that the proposed pilot sites would be the prisons that offer the Earned Release Program, specifically targeting individuals releasing to DCC Region 4.
- The reasons for these recommendations included that these sites were currently offering Evidenced Based, Cognitive Based Substance Use Disorder programming. The current SUD curriculum that is utilized by DAI is Cognitive Behavioral Interventions – Substance Abuse, developed by the University of Cincinnati Corrections Institute. With MAT as an evidenced based approach to treating Opiate Use Disorder, it was imperative to include pilot sites that offer evidence based SUD programming. These pilot facilities also needed to have the capabilities of a Health Services Unit to provide a medical screening and the injection prior to release.
Division of Adult Institutions (DAI) Procedures ( Workflow)
Workflow)
https://doc.wi.gov/Pages/OpioidProgramToolkit/Images/DAIProcess2017.pdf
- Social services staff/case managers screen inmates for eligibility and utilize a data tracking sheet to document throughout the pilot process.
- Documentation of those who decline participation are also recorded for data purposes.
- DCC probation and parole agent is contacted if offender agrees to participate to facilitate continuity of care upon release into the community.
- Medical screening by health services staff is completed and documented accordingly.
- Communication between social services staff/case managers and health services staff occurs to determine if offender is medically eligible to participate in the pilot.
- If offender is not medically eligible, social services staff/case manager documents accordingly on the data tracking sheet.
- If the inmate is medically eligible, the process continues and the DAI pharmacy is contacted to obtain the Vivitrol injection prior to release.
- Inmate is given a urine drug screen in the week prior to the anticipate injection date and the injection is scheduled for up to seven days prior to release.
- Offender is released and the continuity of care is transferred to the probation and parole agent in the community.
- Social Services staff/case managers document on the data tracking sheet and submit for data recording purposes.
Division of Community Corrections (DCC)
Program participants may be serving probation or released to community supervision from county jails or the prison system. Participants must volunteer and meet the criteria of having a current or history of opioid addiction. The following information is provided prior to having the participant begin the program.
- Provide the candidate information about the program and the MAT - Why is the Vivitrol different than other medication assisted treatments?
- It’s a long-lasting injection, which means it’s only administered once per month
- It’s administered by a professional only
- It won’t prolong your dependence on opioids or alcohol
- It doesn’t replace or act as a substitute for opioids or alcohol
- It will not result in withdrawal when you stop taking it
- It’s an opioid blocker/antagonist
- Clarify program expectations
- Required to be opioid-free for a minimum of 7-10 days prior to injection
- Monthly shot administered by a professional
- Attend and comply with necessary AODA treatment
- Graduation ceremony (voluntary)
- Review risks/side effects
- Severe overdose risk if attempts are made to overcome the opioid blocking effect
- Amounts that you used to prior to beginning the shot are more likely to result in overdose and may be fatal
Volunteers must then pass a medical screen, which includes a urinalysis to confirm they are opioid free. The offender is transferred to a Vivitrol Specialty Agent who has been trained in the program. Required paperwork is completed:
Agents schedule first Vivitrol injection/transportation. It is strongly encouraged that agents transport participants to their first injection. This is a critical time and the urge to use may be stronger than their motivation to maintain sobriety.
- When someone is accepted into the pilot program, referrals are made for an AODA assessment and cognitive based programming.
- Alcohol and drug treatment: 8-10 weeks of intensive outpatient followed by 16 weeks of aftercare. Participants are also expected to attend AA/NA meetings to assist in their recovery.
- Cognitive based treatment: 12 week cognitive behavioral program that focuses on decision making.
Urine Screening
Urine screening is an evidence-based practice used in correctional systems to monitor its populations for the use and misuse of controlled and uncontrolled drugs. Wisconsin has a formal process of urine and saliva collections both in our institutions and in the community that is driven by security measures and case planning. As part of our pilot program, participants submit weekly samples in order to:
- Discourage use of opioids
- Monitor for use of other illegal substances
- Increase treatment compliance
- Increase the safety of inmates and program participants
Contact Standards
The structure of supervision during the program is as follows, and may vary depending on an offender’s performance and progress. Supervision standards for these levels are:
- 90 days on enhanced supervision
- Weekly face-to-face contacts
- Home visits every six months
- A minimum of one monthly collateral contact
- Treatment providers should be contacted monthly as part of the case plan and do not represent a collateral contact
- 90 days on maximum supervision
- Face to face visit every 14 days
- Home visits every six months
- 90 days on medium supervision
- Face to face visit every 30 days
- Home visits every six months
Lessons Learned
Lessons Learned from Implementation In DAI Facilities:
- DAI sites were expanded after initial participation numbers were low. It is the impression that offenders participating in the intensive Earned Release Program often thought they were “cured” and did not need Vivitrol when released.
- More staff training and buy-in to the pilot is important and having a plan moving forward for training with staff turn-over, etc.